
How You Sleep Is Shaping Your Spine: A Structural Guide to Sleep Position

We spend a lot of time talking about posture during the day: how you sit, how you stand, how you carry your bag, how you look at your phone. But there's a posture conversation that accounts for roughly eight hours of every single day that doesn't get nearly enough attention: how you sleep.
Think about that for a moment. If you're sleeping seven to eight hours a night, you're spending approximately one third of your life in a single sustained position. For anyone in active structural correction care, that's either eight hours reinforcing the work being done in the office, or eight hours working against it. Sleep posture is one of the most significant structural inputs your body receives every day.
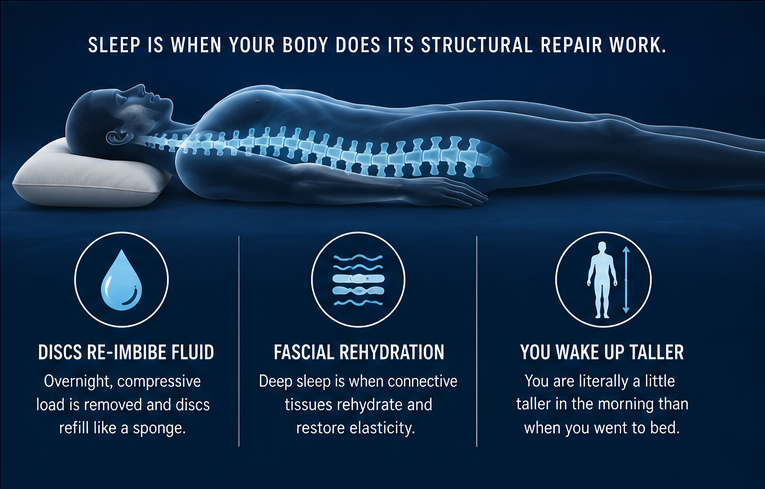
Sleep Is When Your Body Does Its Structural Repair Work
The fascial rehydration and Connective Tissue Restoration work that happens during care is most effective during deep sleep. Beyond that, spinal discs re-imbibe fluid overnight as compressive load is removed in the horizontal position, think of the difference between a wet sponge being pressed down versus one that's unloaded and refills with water. You are literally a little taller when you wake up in the morning than when you went to bed.
The problem is that if you're sleeping in a position that maintains or creates a structural abnormality (forward head, flattened cervical curve, rotated pelvis) your connective tissues are rehydrating and adapting around that abnormal position rather than a corrected one. Over months and years, sleep posture actively shapes your structure, the same way any other sustained posture does. The pockets of dehydrated, adhered fascia we work to address in care often develop precisely because of what the body is doing during those eight hours.
The Three Positions: A Structural Breakdown
Back sleeping: best for structural neutrality
Sleeping on your back allows the spine to decompress in its most neutral position. Gravity distributes evenly across the entire posterior surface rather than concentrating at specific points. The critical variable is pillow height. A pillow that is too thick pushes the head forward, recreating the Anterior Head Syndrome (AHS) position you spend your waking hours working to correct. A pillow that is too flat allows the head to drop back with no cervical support. The goal is a pillow that supports the natural cervical lordosis, maintaining the curve rather than flattening it, while keeping the head aligned with the rest of the spine.
Side sleeping: good with the right support
Side sleeping is the most common position and can be structurally supportive when done correctly. The key is pillow height; it needs to be tall enough to fill the space between your shoulder and your head, keeping the cervical spine level rather than dropping toward the mattress or being pushed up away from it. Shoulder width and mattress firmness both affect the right pillow height, which is why there is no one-size-fits-all answer. A pillow between the knees is also valuable for side sleepers as it prevents the top hip from rotating forward, which reduces torsional stress through the lumbar spine and pelvis overnight.
Stomach sleeping: the worst position structurally
Stomach sleeping is the one position worth making a real effort to transition away from. To breathe while lying face down, you must rotate your head to one side and hold it there for hours. This creates sustained, asymmetric cervical rotation that directly loads the joints, discs, and soft tissues of the neck in a compromised position all night long. It also places the lumbar spine in extension with the abdomen sinking into the mattress. If stomach sleeping is deeply ingrained, the transition takes time, but it's worth making. A practical starting point is placing a pillow under your hip on one side to encourage rotation toward your back or side.

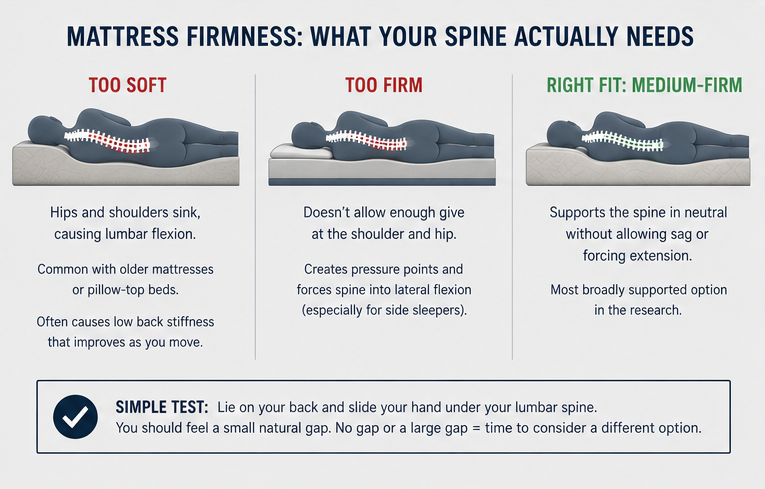
Mattress Firmness: What Your Spine Actually Needs
The mattress firmness debate is long-standing and often overcomplicated. The structural goal is straightforward: the mattress should support the spine in a neutral position without allowing it to sag into flexion or forcing it into extension.
Too soft: the hips and shoulders sink, causing the lumbar spine to bow into flexion for hours. This is common with older mattresses or pillow-top beds. If you wake up with low back stiffness that improves as you move around, this is often the culprit.
Too firm: for side sleepers especially, an overly firm mattress doesn't allow enough give at the shoulder and hip, creating pressure points and forcing the spine into lateral flexion between those contact points.
Medium-firm is the most broadly supported option in the research for spinal neutrality. A simple self-test: lie on your back and slide your hand under your lumbar spine. You should feel a small natural gap. No gap or a large gap means the mattress may not be supporting your structure the way it should.
The Right Pillow Makes a Significant Difference
Most pillows are designed for comfort. What patients in structural correction actually need is a pillow designed for correction, one that supports the cervical curve rather than flattening it, and maintains proper head alignment whether sleeping on the back or side.
At Structural Chiropractic, we now carry the Denneroll Pillow, the only pillow specifically engineered to support cervical lordosis correction during sleep. For back sleepers, it positions the head to eliminate forward head posture while an insert actively creates cervical lordosis overnight. For side sleepers, the contoured shape provides two different heights of neck support to accommodate shoulder width and mattress density. It's available in three sizes (large, medium, and pediatric) and the right fit is determined by shoulder width and mattress density.
If you've been working consistently on your correction during visits and doing your self-care, but returning each night to a pillow that puts your cervical spine back into a compromised position, you're working against yourself for a third of your life. Ask about the Denneroll at your next appointment.
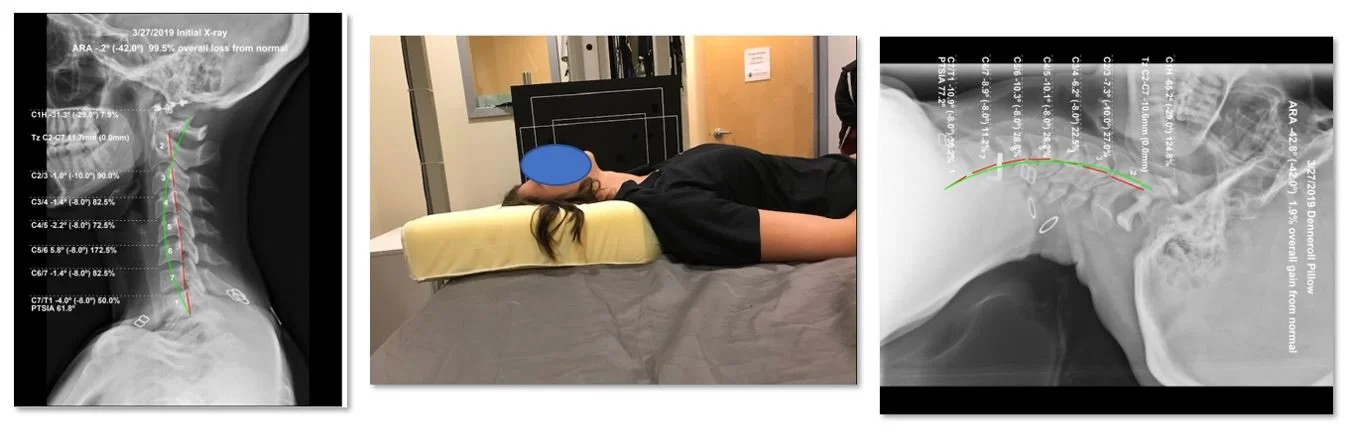
Left: Initial cervical X-ray showing significant loss of cervical lordosis. Center: Patient positioned on the Denneroll Pillow. Right: X-ray taken while patient is actively lying on the Denneroll Pillow. (source)
Sleep Is a Structural Tool
Sleep is one of the most powerful and most underutilized inputs in your structural correction plan. Position, pillow, and mattress are all part of the puzzle and getting them right doesn't require a complicated protocol as much as intentional choices.
If you have questions about your sleep position or how it relates to your structural correction call us at (412) 835-4844, visit structuralchiropit.com, or tape the button below to schedule your complimentary consultation.